
Physiology of the aorta
The aorta is the large tube that connects the heart to the rest of the body. Its job is to deliver oxygen in the blood from the heart to the body. The size of the aorta is directly proportionate to the patient’s height and weight, and its diameter may range from 1.2cm (half an inch) to 3cm (more than an inch).
The aorta is divided into three sections:
- Ascending aorta, which rises out of the left ventricle and supplies the heart with blood through the coronary arteries.
- Aortic arch, which arches over the heart (like an upside down "U"), giving rise to branches that bring blood to the head, neck, and arms
- Descending aorta: Thoracic aorta, which travels down through the chest and supplies blood to the ribs and some chest structures. Abdominal aorta, which begins at the diaphragm and provides blood to most of the major organs of the abdomen through its branches. In the lower abdomen, it ends in a bifurcation into the left and right common iliac arteries, which supply blood to the pelvis and the legs.
The aorta is an elastic artery, and as such is quite capable of widening. It consists of a mix of smooth muscle, nerves, and cells. Like all arteries, the aortic wall is made up of three layers:
- Inner intimal layer: provides a smooth surface for blood to flow across
- Middle medial muscular and elastic fibre layer: allows the aorta to expand and contract with each heartbeat
- Outer adventitial layer: includes vessels (vasovasorum) supplying the aortic wall with oxygenated blood, and provides additional support and structure to the aorta.
![]()
![]()
![]()
![]()
Figures (left to right): Normal aorta, Ascending tear (90%), Arch tear (5%), Descending tear (<5%)
Diseases of the aorta
Acute and chronic aortic disease
Acute aortic dissection (figure one) is a tear in the inner lining of the aorta. The tear creates a false channel, creating a double-barrelled tube in which the blood flows through the middle of the muscle, compromising where the blood should normally flow. It causes a significant weakness and the potential for it to rupture (figure two).
Figure two: pathogenesis of dissection
![]()
![]()
![]()
Less common types of acute aortic disease are penetrating atherosclerotic ulcer (PAU) and intramural haematoma (IMH). Both of these conditions can lead to an aortic dissection (figure three).
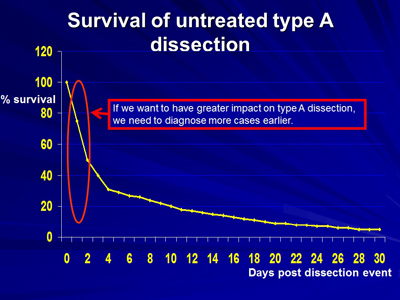
Dissections less than two weeks old are referred to as acute. Those greater than two weeks are known as chronic. Acute aortic dissections must be treated urgently based on the patient’s condition (figure four).
Figure three: acute aortic syndromes
![]()
![]()
![]()
![]()
Figure four: Survival rates
Download the full size image.
{kind=link}
Acquired aortic disease
Acquired heart diseases are conditions that develop over a person’s lifetime, in contrast to inherited, which are present at birth. Approximately 50 to 75 per cent of patients will have evidence of hypertension or a previous diagnosis. Other risk factors include smoking and raised cholesterol.
Inherited heart disease
Inherited or congenital heart disease is present at birth. Normally, cardiac abnormalities are caused by abnormal development of the heart and circulatory system while in the womb. They can be caused by a variety of factors, including infection and use of certain drugs during pregnancy. Some congenital cardiac abnormalities are inherited and may be transmitted. However, for some people there is no obvious relationship nor is the origin of the disease readily explained.
Inherited heart disease can include Marfan syndrome, Ehlers-Danlos syndrome and familial thoracic aortic aneurysm type 1 and 2.
The condition known as bicuspid aortic valve (BAV) can also be a risk. It is by far the most common cardiovascular abnormality, occurring in one or two percent of the general population. Typically, patients have no symptoms in earlier life but the aortic valve becomes narrowed and begins to obstruct the flow of blood from the heart to the rest of the body when the patient reaches middle age (around 50 years old)
In approximately one-third of patients, there is an associated weakness of the aorta which causes a swelling of the aorta (an aneurysm) later in life.